Stereotactic radiosurgery (SRS) and stereotactic radiotherapy (SRT) for brain tumours
Stereotactic radiosurgery and stereotactic radiotherapy are types of brain tumour treatment. They use radiotherapy beams that precisely target the tumour. They are non-invasive types of treatment that are effective at targeting tumour cells while reducing damage to healthy cells.
On this page:
- What are stereotactic radiosurgery and stereotactic radiotherapy?
- What does receiving stereotactic radiosurgery and stereotactic radiotherapy treatment involve?
- Can I have stereotactic radiotherapy?
- Helping you prepare for radiotherapy
- Listen to others’ personal experience
- If stereotactic radiotherapy doesn’t work
Get your free Information Pack
Our Brain Tumour Information Pack can help you better understand your diagnosis and feel confident talking to your medical team.
Make the right choices for you
Our Step by Step interactive guide outlines what happens following a diagnosis, to answer your questions and help you to understand what to expect.
Join our online support groups
Our online support groups are a great place to connect with other people affected by a brain tumour.
What are stereotactic radiosurgery and stereotactic radiotherapy?
Stereotactic radiosurgery (SRS) and stereotactic radiotherapy (SRT) use highly focused beams of radiation to target treatment to brain tumours.
With stereotactic radiosurgery and stereotactic radiotherapy, healthcare professionals can accurately point lots of narrow beams of low-dose radiation at the tumour. They do this from different angles around the head. Using lower-doses of radiation means each beam causes less damage to healthy brain tissue that it passes on the way to the tumour.
Stereotactic radiosurgery is usually delivered in one outpatient appointment, while stereotactic radiotherapy is normally delivered in 3 or 5 outpatient appointments.
Computed tomography (CT) or magnetic resonance imaging (MRI) images are used to accurately find and see tumours within the brain. CT uses X-rays to produce the images while MRI uses huge magnets. Your healthcare team might need both types of brain scans for treatment. This is common.
The beams are precisely targeted so they overlap at the site of the tumour. Then the low doses of radiation combine to destroy the tumour cells.
Stereotactic radiosurgery and stereotactic radiotherapy can be delivered using a number of different technologies and platforms. So you may hear different terms used by your medical team. They include Gamma Knife®, CyberKnife® and specially configured linear accelerators (LINACs).
What does receiving stereotactic radiosurgery and stereotactic radiotherapy treatment involve?
Much of the stereotactic radiosurgery and stereotactic radiotherapy procedures are similar to conventional radiotherapy and they use the same type of radiation.
During the treatment it’s vitally important that your head is as still as possible to make sure that the radiotherapy beams accurately reach the tumour cells rather than healthy cells.
This is even more important if you’re receiving fractionated stereotactic radiotherapy (FSRT), as your head needs to be in the same place for each treatment, so the narrow beams target the same area each time. This requires a lot of careful planning before your treatment can start.
The planning stages
Firstly, your medical team will make a device to keep your head still during treatment. This is made just for you. There are two main ways of achieving this.
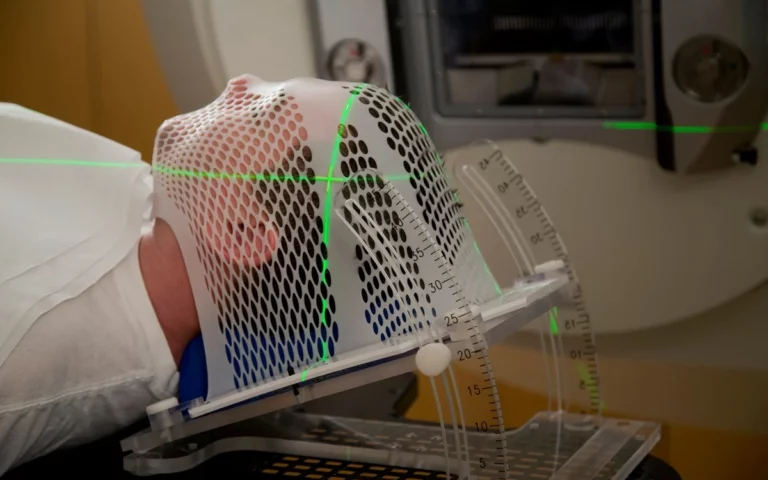
Stereotactic mask
Similar to the mask used in conventional radiotherapy, this is often made from a type of plastic called thermoplastic. The mask has holes in it so you can breathe. You only need to wear this during your planning scan or when you go for treatment.
To create the mask, a sheet of plastic mesh that has been softened in warm water, is placed over your face and head. The mesh is then moulded to closely fit your individual head-shape and, as it cools, the mask hardens. The entire process can take up to 45 minutes.
Because a stereotactic mask needs to be a closer fit than a conventional radiotherapy mask, men with facial hair may need to shave before the mask is made. The hair on your head doesn’t need to be shaved, but if you’re planning a haircut, it should be done before your mask is made. Your hair should also be clean and product-free.
Once the mask is ready to wear, you’ll usually have an MRI scan without the mask and then a CT scan wearing the mask. The specialists use both of these diagnostic scans together to help build a 3D picture of your tumour and plan your treatment accordingly.
The specialists will work out from the scans exactly where the tumour is and how to aim the beams. You’ll often be asked to return to the planning team to have the positioning checked before going on to treatment.
Head frame
You often use head frames during stereotactic radiosurgery and stereotactic radiotherapy and, although they may look scary, they’re actually lightweight. You will not have hair shaved during treatment, but it should be clean and product free.
Depending on the equipment used during the treatment you may need a head scan so that treatment staff can make a frame that fits you – this can take most of a day. In other cases, the frame will be fitted straight away and measurements taken with a special ruler. Your radiographer will explain the process to you.
The experts will attach the frame through your skin to the surface of your skull using four small pins and this should take about ten minutes. You’ll receive local anaesthetic by injection at the points where the frame will be attached. This can cause some discomfort until the anaesthetic takes effect and you may also feel some tightness or pressure. These areas will likely be sore afterwards.
Once experts complete fitting the frame, you’ll have another scan to allow your healthcare team to plan your treatment and set up the machine to precisely target your tumour.
This planning stage can take several hours, during which time you can get something to eat or drink. You continue to wear the head frame throughout this process, which can be quite tiring. Your radiographer can arrange for you to have some light pain relief if you find wearing the frame uncomfortable.
Once the medical team finish with the planning, you’ll receive your treatment and experts will remove the head frame when the treatment is over.
The procedure
Stereotactic radiotherapy (SRT) and fractionated stereotactic radiotherapy (FSRT)
During stereotactic radiotherapy and fractioned stereotactic radiotherapy treatment, you’ll lie on the treatment couch, and the radiographers will position you correctly. Your health team will fit your treatment mask over your face and attach it to the couch. This usually takes just a few minutes, but can take longer if the treatment is particularly complex.
Before the treatment begins, medical staff will leave the room, but they’ll be able to see and hear you. You’ll also be able to hear them and they’ll guide you through the process.
Some patients find music helps them to relax during the treatment. And your radiographers can arrange this for you.
The machine that your medical team will use during the treatment is called a linear accelerator (LINAC). This is similar to a large X-ray machine and its purpose is to give standard radiotherapy to many different parts of the body.
The LINAC moves around your head delivering numerous beams of radiation from different angles. The beams all overlap at the site of the tumour. They create a high dose of radiation and destroy the tumour cells.
You might also hear about CyberKnife®, which is a similar machine. This is essentially a LINAC machine that has been specifically designed to give stereotactic radiotherapy and fractionated stereotactic radiotherapy. It has a small linear accelerator on a robotic arm, which moves around your head delivering the radiation. It also tracks any movements the patient makes and adjusts its positioning before continuing with treatment.
There’s currently no identified advantage of using one machine over another.
Treatment itself only takes around 20-40 minutes with a LINAC machine or 30-90 minutes with a CyberKnife®. However, you’ll be at the hospital for some time as it takes a while for the radiographer to fit your mask, attach it to the table and position you correctly.
Usually, once your treatment has finished, you can go home. It’s advisable to arrange transport, as you may feel too tired to drive safely.
You’ll need to return to the hospital several times to have your course of treatment. The number of treatment sessions you’ll need will depend on your treatment plan. But fractionated stereotactic radiotherapy can typically take around 5-25 sessions.
Stereotactic radiosurgery (SRS)
treatment is much the same as fractionated stereotactic radiotherapy. The big difference being that the delivery of the treatment is in just one session.
Either before treatment begins or shortly afterwards your doctor may give you steroids to reduce brain swelling or anti-seizure drugs to help prevent a seizure.
You’ll lie on the treatment couch and the radiographer will position your head by attaching the frame to a support on the couch. Then the radiographer will adjust the couch and the treatment machine into place before the treatment begins.
The staff will leave the room, but will be able to see and hear you, and you’ll be able to hear them.
In addition to using LINAC machines or similar equipment designed specifically to treat the brain, SRS treatment may use a machine called GammaKnife®.
GammaKnife® uses gamma rays rather than X-rays to target and treat the tumour. It’s important to note that this is still radiation and does not involve an actual knife. The machine looks quite different to a linear accelerator, but the preparation, delivery and outcome are much the same.
Stereotactic radiotherapy treatment is likely to take longer than fractionated stereotactic radiotherapy and may take up to four hours. The time taken depends on the size of the tumour, the radiation dosage and the machine used.
When the treatment has finished, the treatment staff will take you out of the machine and remove the head frame. Then they will monitor you for a while. And, in some cases, your doctor may want to admit you to the ward for monitoring overnight.
After treatment
After treatment you’ll have regular appointments with your doctor or specialist nurse. During these appointments you’ll be able to talk about your recovery. And it’s important to discuss any symptoms or side-effects you may be experiencing.
If you’re concerned about any side-effects, you should speak to your medical team rather than wait until your next scheduled appointment.
It’s important to note that DVLA regulations mean you’ll need to stop driving for a period of time following your treatment. This period can vary and your consultant should tell you which restrictions apply to you.
If you work, it is likely that you will have to take some time off work during treatment and for a short time afterwards. Our employment resources provide help and information on how to approach your employer about your diagnosis. And how they can support you through this time.
We run a benefits and money clinic twice a week to help people affected by a brain tumour access the financial support they’re entitled to. As well as providing expert guidance on how they can make the most of their money.
Can I have stereotactic radiotherapy?
Stereotactic radiotherapy is not suitable for all types of brain tumours. It is generally for patients with small tumours that are less than 3cm at the widest part.
The beams of low-dose radiation that medical experts use in SRT are able to damage tumour cells when they overlap with each other to create a higher dose of radiation. Because these beams are very narrow, the area where they overlap is very small.
To create that higher dose of radiation across a larger area would require more beams of radiation.
Each beam has to travel through some healthy brain tissue and using more beams would do more damage to the healthy tissue. This would likely result in areas of dead tissue known as radiation necrosis, which can cause swelling of the brain (oedema) and the development (or worsening) of cognitive difficulties.
To prevent necrosis, patients with larger tumours (usually 3cm and above) would have to have treatment with even lower doses of radiation that may not effectively destroy the tumour. So, the advantage of stereotactic radiotherapy over conventional radiotherapy would therefore disappear.
SRT is suitable for treating:
- small low grade tumours with an obvious edge
- haemangioblastomas that couldn’t be completely removed or which came back after surgery
- other small low grade tumours, like acoustic neuromas, pituitary adenomas and chordoma or meningiomas at the base of the skull
- secondary brain tumours that have developed somewhere else in the body and migrated to the brain.
SRT may not be suitable if the treatment area includes certain important nerves, as they may receive too much radiation and become damaged.
In some cases, conventional radiotherapy is more appropriate as not all brain tumours benefit from stereotactic therapy.
Healthcare professionals make the decision to treat with SRT on a case by case basis. Your oncologist will discuss your treatment options with you and the wider members of your multi-disciplinary team (MDT) to come up with the treatment plan that is best for you.
Additionally, SRT isn’t available in all hospitals as they require specialised equipment and staff. This issue is currently under review by the government and the NHS.
However, there are centres that can deliver SRT for brain tumours in all four countries of the UK. In England, there are services to make sure that patients in all areas of the country have access to SRT for illnesses such as brain tumours and metastases.
SRT may also be available privately and you should speak to your health team to find out more.
Helping you prepare for radiotherapy
Listen to others’ personal experience
In this episode of our podcast ‘Let’s Talk About Brain Tumours’ we talk to Andy and Katie about Stereotactic Radiotherapy. Both Andy and Katie had this treatment when they had a recurrence of their brain tumours. They explain what the treatment entails and what it was like to undergo.
Despite the word ‘knife’ appearing in the names Gamma Knife® and Cyberknife®, there’s no actual knife used. The reason behind this name is because the neurosurgeon who invented it. Professor Lars Leskell, felt that the treatment allows high levels of precision – like a surgeon’s knife.
Stereotactic radiotherapy (SRT) refers to two different ways of delivering the treatment:
- Fractionated stereotactic radiotherapy (FRST), which patients receive over multiple sessions
- Stereotactic radiosurgery (SRS), which patients only receive in one session and, despite its name, doesn’t involve actual surgery.
Unless otherwise specified, when we refer to SRT we mean both FRST and SRS.
Although some types of conventional radiotherapy, deliver beams of radiation from various angles around the head, stereotactic radiotherapy uses more angles and better images to target tumours more accurately.
Thanks to this accuracy, healthcare professionals can target a smaller area around the tumour. This means that less healthy tissue gets the high dose of radiation, so it is less affected and can recover. This also means that a higher dose can safely be given to the tumour, or that fewer treatment sessions may be needed.
As a result, people generally experience fewer side-effects with stereotactic radiotherapy compared to conventional radiotherapy.
If stereotactic radiotherapy doesn’t work
Although healthcare professionals develop treatment plans carefully to be as effective as possible. While having the fewest risks or side-effects, sometimes stereotactic radiotherapy may not work. This can be worrying, but just because one treatment hasn’t worked, it doesn’t mean others won’t.
Find out more about what happens when treatment doesn’t work.
Support and Information Services
Research & Clinical Trials Information
You can also join our active online community.
In this section

Get support
If you need someone to talk to or advice on where to get help, our Support and Information team is available by phone, email or live-chat.
Recommended reading
Share your experiences and help create change
By taking part in our Improving Brain Tumour Care surveys and sharing your experiences, you can help us improve treatment and care for everyone affected by a brain tumour.